This page is based on the landmark work by Dr Viotti in Fertility & Sterility, where you can look up the scientific background.
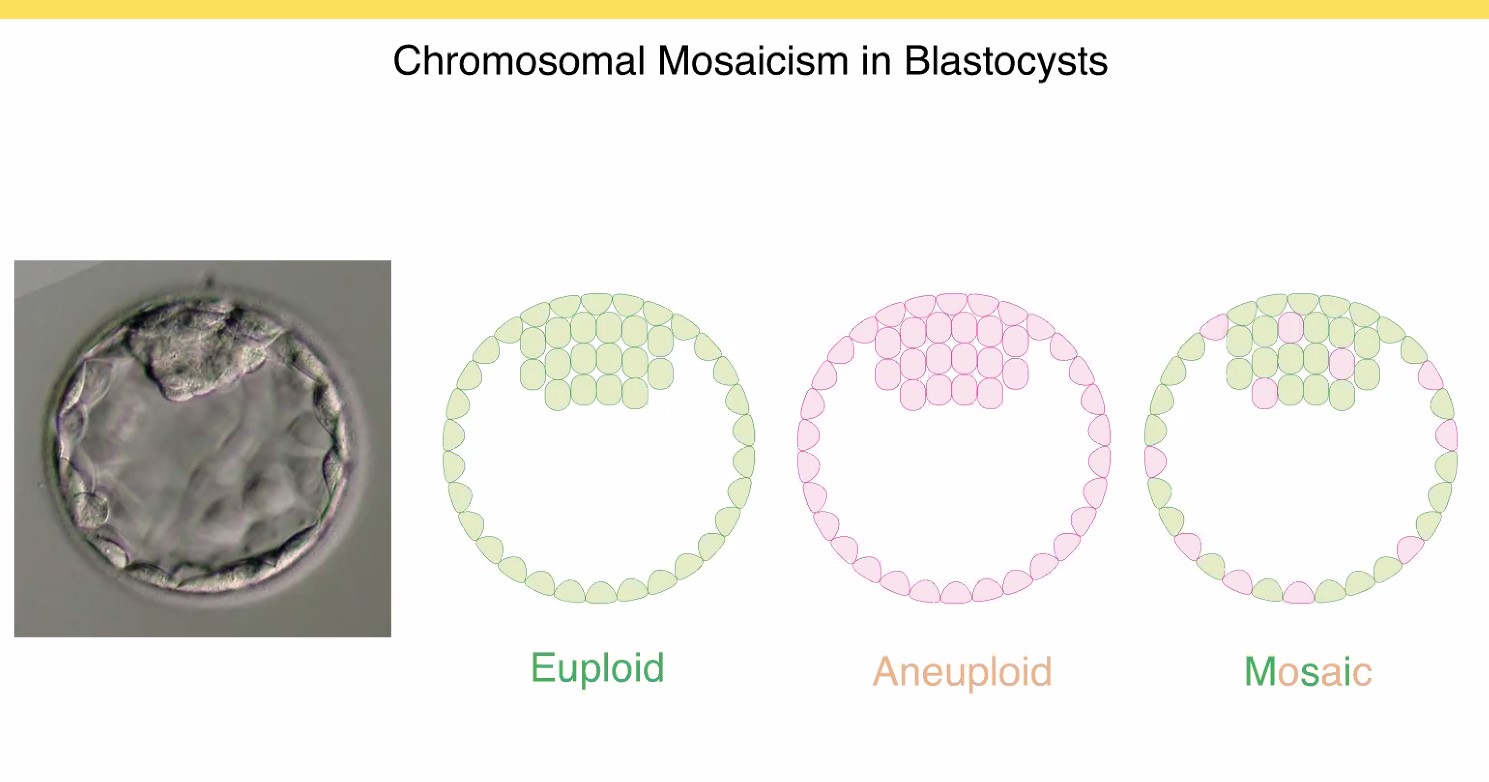
By using preimplantation testing for aneuploidy (PGT-A) on a larger scale, we have learnt that there exists an intermediate category of embryos (blastocysts) with a mixture of normal cells with two copies of each chromosome (green) and abnormal cells with either one or three copies (red), termed monosomy for one copy and trisomy for three copies. This seems to be a normal state of transition for certain blastocysts, because if the red cells are in a minority, they will be eliminated later on, or they are confined to the placenta (a common occurrence) while the baby is perfectly healthy.
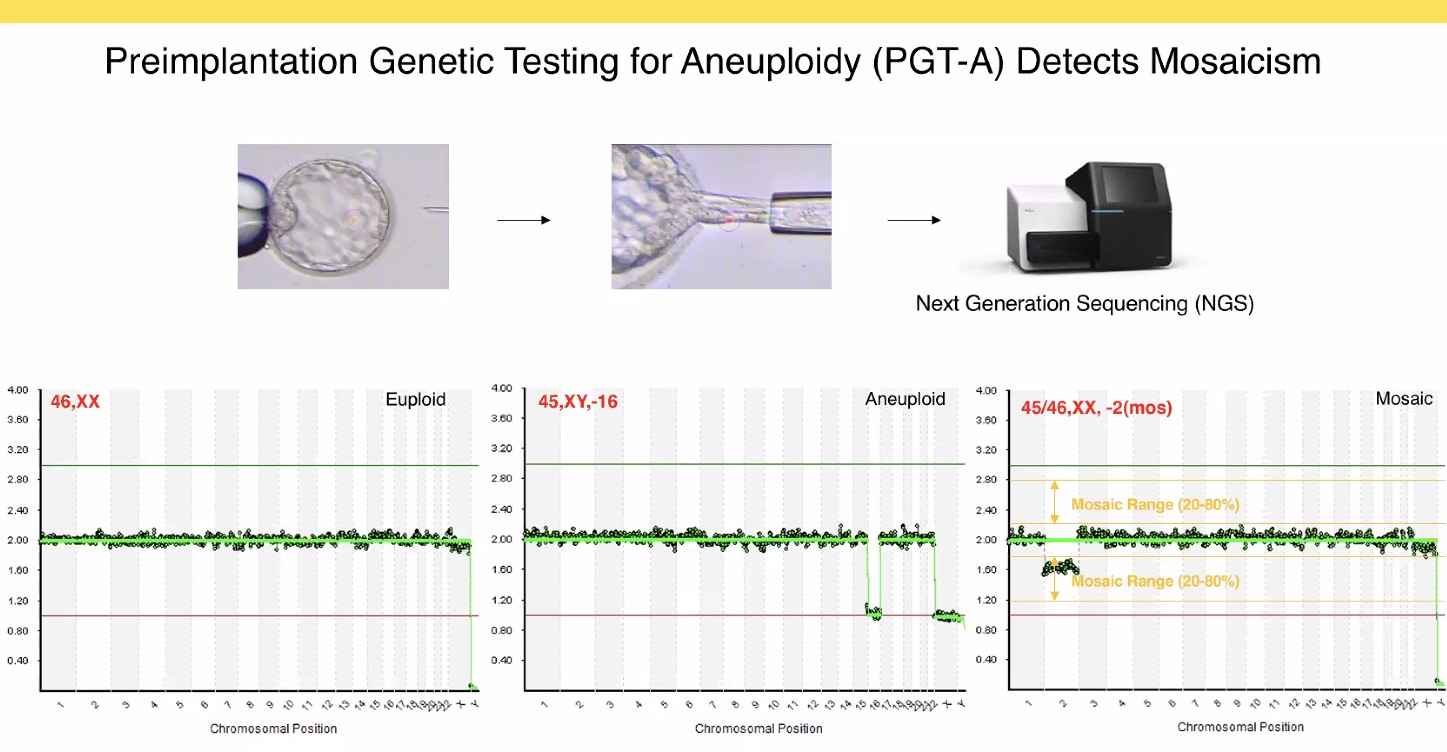
In the laboratory, this produces chromosome signals somewhere in-between the clear-cut 1 (monosomy), 2 (normal) or 3 (trisomy) copies. It is increasingly preferred to call this situation «intermediate copy numbers» than «mosaic». The reproductive potential of a blastocyst depends on the percentage of abnormal cells (where <50% is called «low-grade» and can produce success rates similar to normal embryos) and on the number of chromosomes involved.
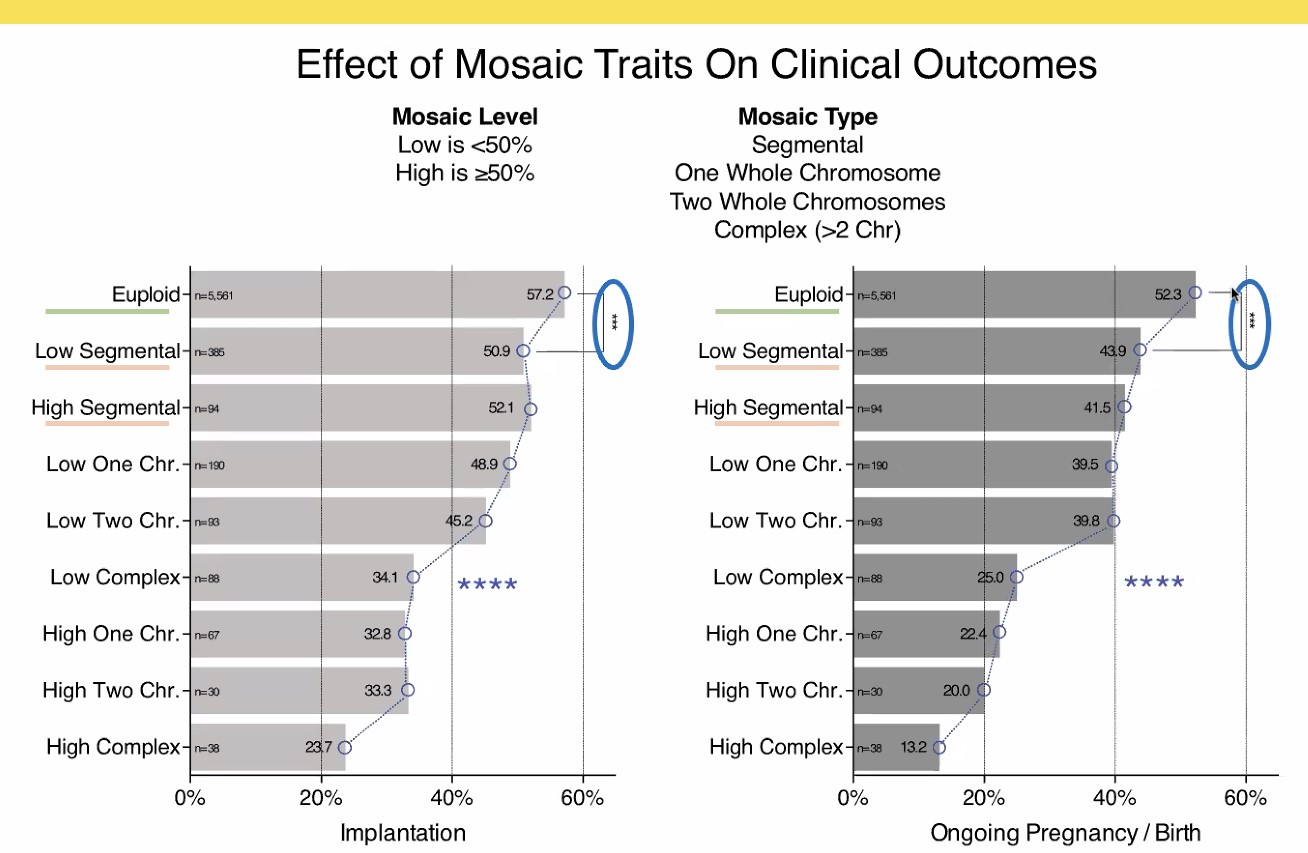
Obviously, the best situation is a completely normal embryo with two copies of each chromosome, with 52% of live births in this series (this is comparable to our own figures). But a low-grade «mosaicism» involving one ore two chromosomes produces around 40% live births after all, which - in the age group of women over 38 - is still way more than in treatments with untested embryos.
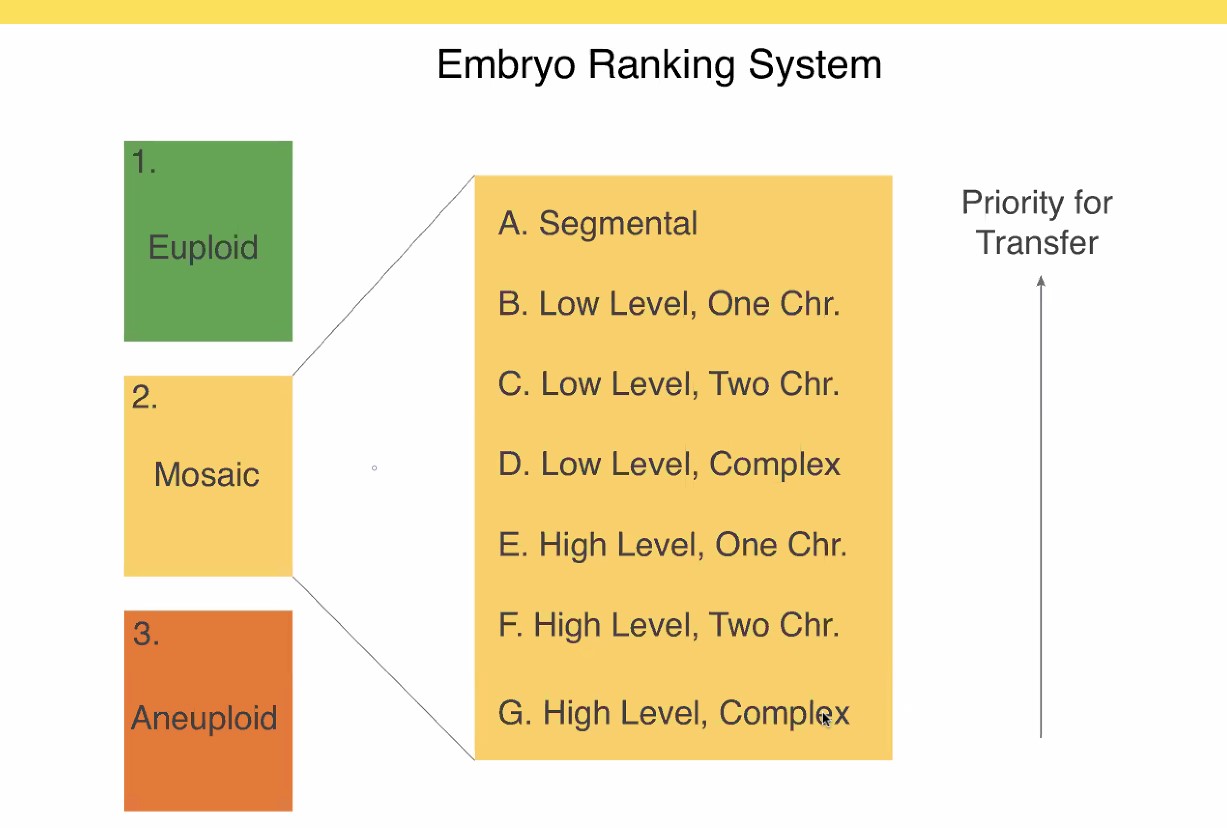
Thus we are left with this traffic light where the intermediate yellow category does clearly improve the overall success of PGT-A, if a woman has no normal (green) embryo available. Carefully selecting those «mosaic» embryos from the yellow group can make the difference between having a baby or not.
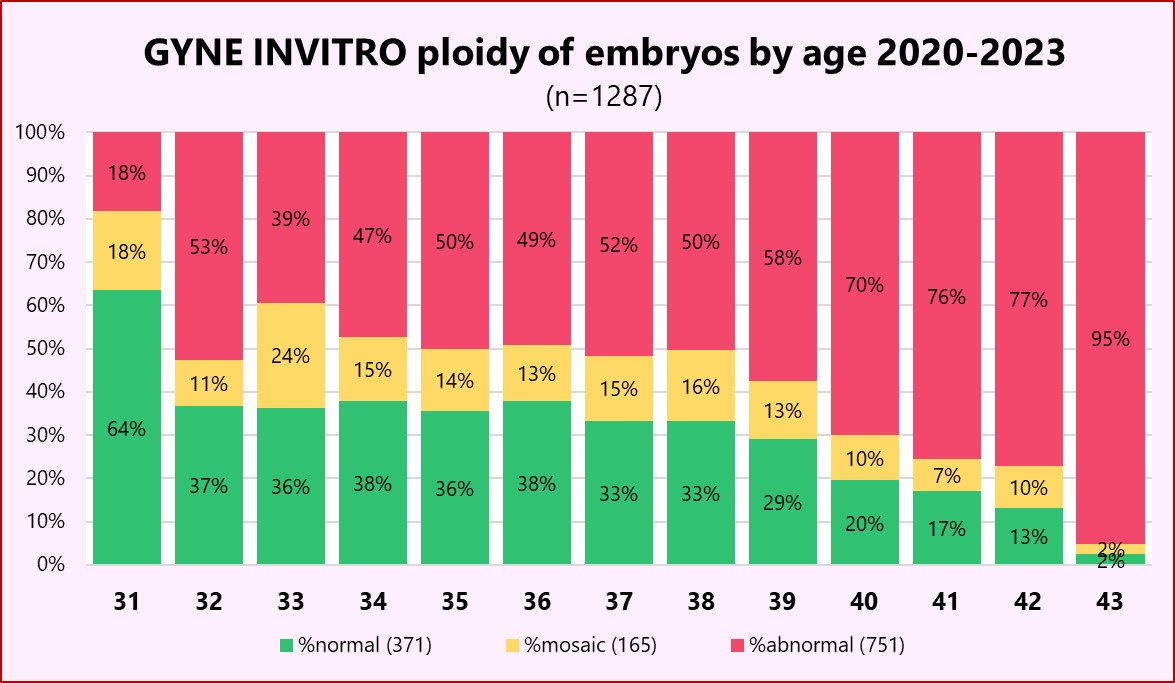
In our GYNE INVITRO laboratory (above), we have acquired significant expertise and experience with PGT-A, and can confirm how age-dependent the proportion of genetically normal embryos is. For women between 35 and 40, the yellow «mosaic» category can contribute significantly to treatment success.
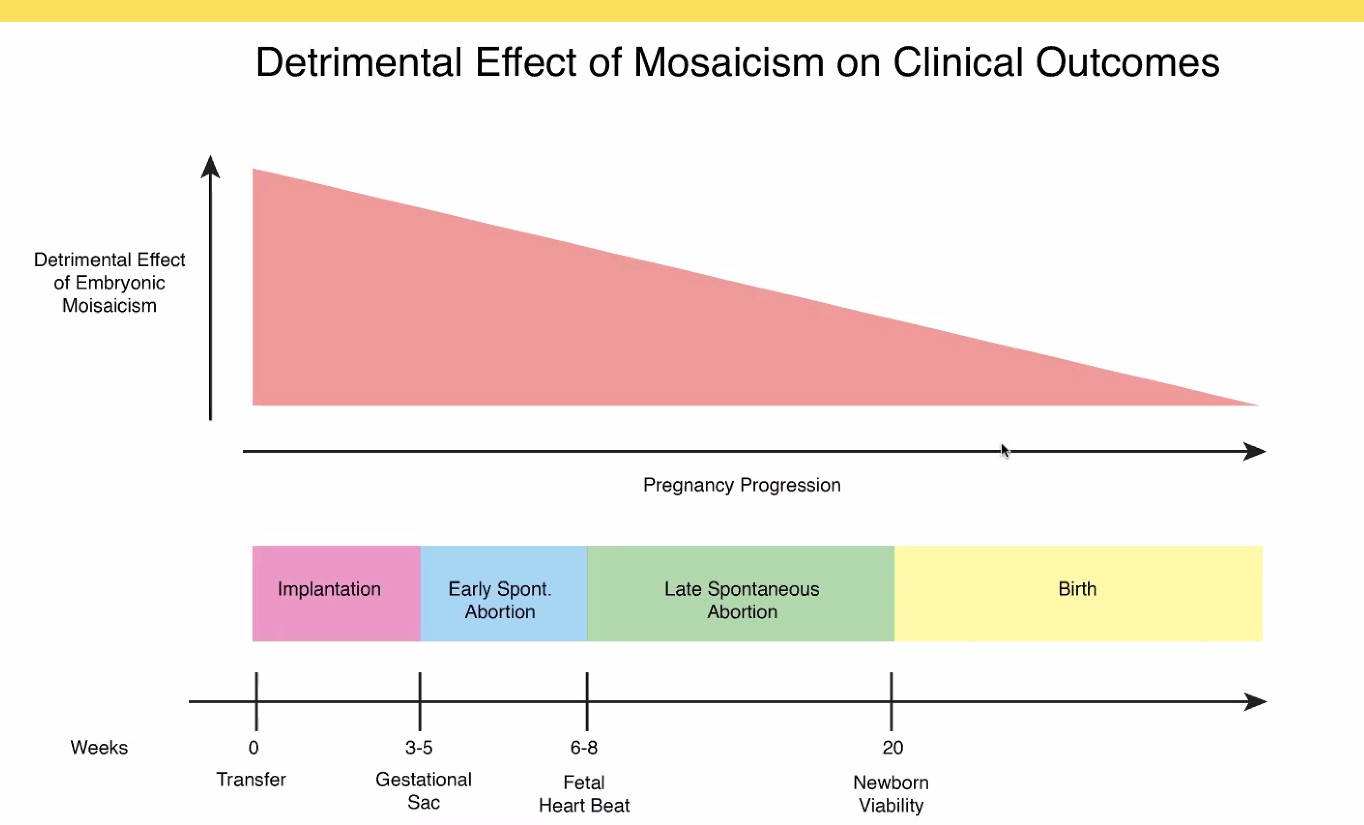
Most importantly, according to available data on thousands of «mosaic» blastocysts, mosaicism does not produce genetic problems in the newborn. The downside of mosaic embryo transfers is merely a reduced success rate in early pregnancy with increased occurrence of miscarriages, but, as mentioned, still above the outcomes of untested embryos.
Couples in need of more in-depth genetic counselling are referred to the international specialist PD Dr Bernard CONRAD and his team in Bern.